The Clinical Director role is one of the strangest jobs in the NHS. Part GP partner. Part service manager. Part workforce lead. Part politician. No clinical training prepares anyone for the political workload. Most CDs do the job for a year or two and step down with a clear view of what would have helped.
This piece sets out the pressures that consume the time, the structural fixes that work, and where outside support changes the day-to-day.
The role on paper
The Network DES specifies the CD as the named clinical leader of the PCN. Required time commitment ranges from 0.5 to 2 sessions a week, paid out of PCN core funding. The role covers clinical service delivery across the network, workforce decisions for ARRS roles, peer relationships between member practices, and the PCN’s interface with the ICB.
That is the description. The actual job is wider.
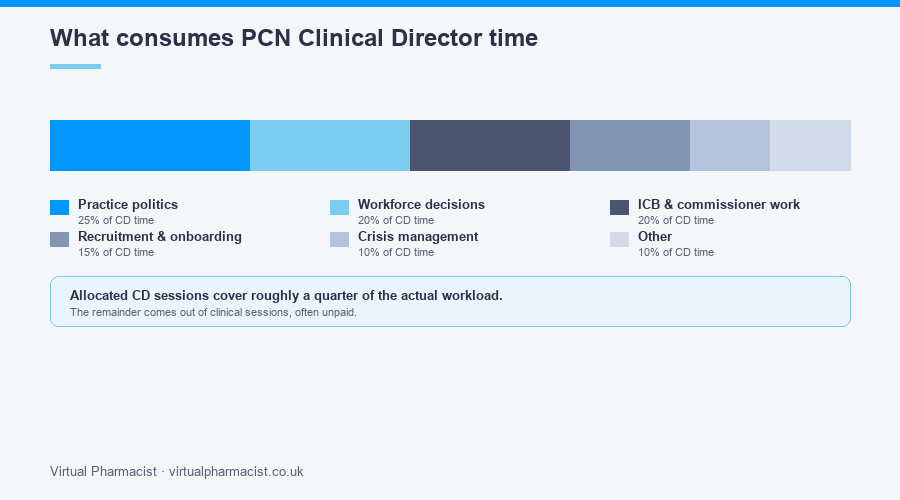
The pressures that actually consume the time
Practice politics. Six practices in a PCN means six sets of partners, six clinical lead voices, six histories with each other. Disputes over patient allocation, ARRS pharmacist sharing, premises decisions, premises money, capitation differences. The CD chairs the room. The CD also delivers the bad news afterwards.
Workforce decisions. Which ARRS roles to recruit. Which practices get the first pharmacist. How supervision is shared. What happens when a role leaves mid-year and the reimbursement schedule shifts. The decision sits with the CD.
ICB and commissioner-facing work. Funding bids. Service redesign meetings. Quality assurance returns. Innovation funding applications. CQC alignment with PCN-level services. None of this is in the job description in detail. All of it lands on the CD.
Recruitment and onboarding. New ARRS roles. Replacing departing staff. Sign-off on contracts. Initial induction. The CD’s name is on the paperwork.
Crisis management. A safeguarding concern raised against a PCN staff member. A patient complaint that crosses practices. A whistleblowing event. Each one is a multi-day distraction.
The hours allocated to the role usually cover a quarter of the actual time it consumes. The remainder comes out of GP partner sessions, often unpaid.
Where the role breaks
Three patterns recur.
CD burnout. Sustained months of working at one and a half to twice the allocated sessions, while still trying to deliver GP clinical sessions. By month 14, attendance at PCN meetings becomes the first thing to slip. By month 18, the resignation is on the table.
Partner relationship damage. A CD who has had to deliver enough hard decisions across six partnerships ends up with strained relationships in their own practice. The home practice no longer wants them taking the role.
Drift. The PCN does what it has always done because the CD does not have the bandwidth to drive change. The annual PCN plan repeats the previous year’s, with the same gaps.
What good CD support looks like
The CDs who survive and deliver tend to have three things in place.
A PCN manager. Not a partial-FTE add-on. A named, paid-for PCN manager who handles the operational lift. The CD chairs strategic discussions. The manager runs the day-to-day.
Defined supervision for ARRS staff. A senior clinician separate from the CD who holds the supervision responsibility for the pharmacist, technician, social prescriber, and care coordinator cohort. The CD oversees. The senior clinician supervises.
Outsourced specialist work. ARRS pharmacist deployment, innovation funding bids, service evaluation. Areas where the work is specialist enough that internal capacity is rarely the right choice.
What to outsource
Three areas account for most of the gains.
ARRS pharmacist and technician deployment. The legwork of recruitment, supervision, governance, payroll, and clinical oversight is significant. An external partner takes the operational work and leaves the CD with the strategic call.
Innovation funding. Bid writing and project delivery are specialist skills. The CD’s time is more valuable on patient and partner-facing work than on grant applications.
Service evaluation. Required for ARRS reporting and innovation funding. Specialist data work. Almost always better done externally than internally.
Where we help
We work with PCNs to take the operational layer off the Clinical Director. ARRS pharmacist and technician deployment, supervision, governance, and reporting under one managed service. Innovation funding and service evaluation as separate workstreams.
Our PCN management support service covers the CD support side. Get in touch for a conversation.