Pharmacy technicians have been on the ARRS list since the role’s introduction. The number of practices that deploy one well is smaller than the number with one on the books. The role description sounds administrative. The good ones are not.
This piece sets out what a technician is, what they can run independently, where they free up pharmacist and GP time, and the deployment patterns that turn the role into a glorified prescription clerk.
What a technician is and is not
A pharmacy technician registered with the GPhC has completed a level 3 qualification, two years of pre-registration practice, and ongoing CPD. They are clinically qualified. They are not pharmacists. They cannot run medication reviews. They cannot make prescribing decisions.
What they can do, with appropriate training and supervision, is run the operational layer of medicines management. Repeat prescription processing. Hospital discharge reconciliation. Audit data extraction. Patient contact about routine medicines issues. Specific medication-related clinics under protocol.
What technicians can run independently
Six pieces of work move cleanly to a technician.
Repeat prescription processing. Authorising routine repeats against agreed criteria. Identifying patients due for review and routing them to the pharmacist or GP. Removing items no longer prescribed.
Hospital discharge reconciliation. Checking discharge letters against existing prescriptions. Identifying changes. Flagging clinically significant changes to the pharmacist. Updating prescribing records.
High-risk drug administration. Sending bloods reminders. Generating phlebotomy forms. Following up missed appointments. Updating the practice register.
Compliance and dosette work. Liaising with community pharmacy on dosette supply. Identifying patients who would benefit from compliance aids. Handling the paperwork.
Specific audit work. Pulling lists for prescribing audits. Cross-referencing prescribing data against guidelines. Producing audit reports.
Patient contact for routine queries. Answering questions about generic switches, supply problems, side effect concerns under protocol, repeat ordering, hospital prescriptions.
Where technicians free up pharmacist time
The unspoken rule of clinical pharmacist deployment in general practice is that the pharmacist’s time is worth most when they are doing prescribing-level clinical work. Every hour of pharmacist time spent on repeat authorisation or discharge reconciliation is an hour not spent on medication review or high-risk drug management.
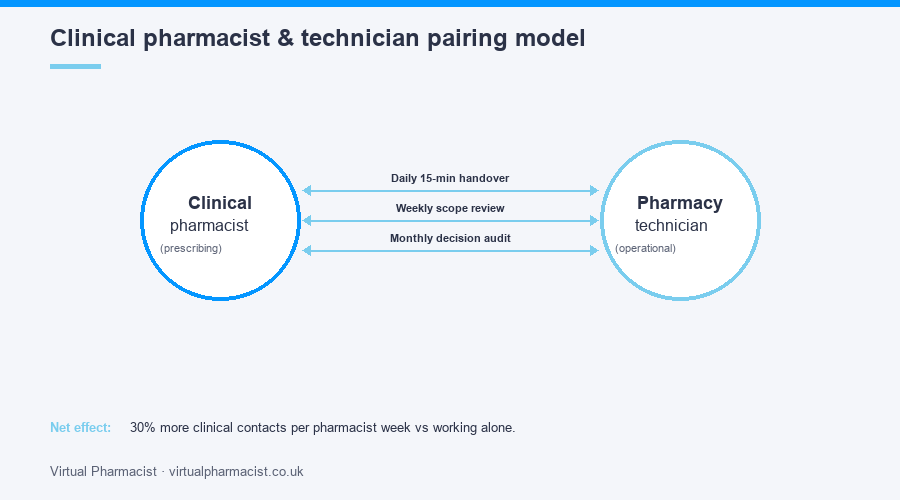
A technician absorbs the operational layer. A clinical pharmacist with a technician partner runs roughly 30% more clinical contacts per week than the same pharmacist working alone.
In a six-practice PCN, the typical configuration is two clinical pharmacists and one full-time technician. Some PCNs run two-to-one ratios in either direction. The point is the pairing, not the precise ratio.
The deployment mistakes
Technician hired with no protected supervision. The role needs a named clinical supervisor (a pharmacist or senior pharmacist) and protected time for the supervision to happen. Practices that skip this end up with a technician working blind on tasks that need clinical oversight.
Technician used as a general admin. Front-line phone work. Booking appointments. Scanning. Filing. The role goes the way of any other administrative role and the medicines work it was meant to absorb stays with the pharmacist.
No agreed scope of practice. Without a written list of what the technician can authorise independently, every decision becomes a question to the pharmacist. Net time saved: zero.
Hired the wrong band. A technician straight out of training cannot run the operational layer of a busy practice without daily supervision. A senior accuracy-checking technician with five years of clinical pharmacy experience can.
Pairing technicians with pharmacists
The pairing model that works is straightforward.
Daily quick-fire handover, 15 minutes. What the technician picked up. What needs clinical input. What the pharmacist is working on. What is parked.
Weekly review of the agreed scope. Has anything new come up that needs to be added to the scope or escalated out of it?
Monthly audit of decisions. A sample of decisions the technician made. The pharmacist reviews for clinical safety. Adjustments to scope follow.
This pattern keeps the technician growing in scope without the pharmacist needing to supervise every individual decision.
Getting the role right
The practices and PCNs that get the most from their technician role tend to do three things on day one.
Write the scope of practice as a one-page document and put it on the technician’s desk. Update it quarterly.
Pair the technician with a named pharmacist supervisor, not a rotating group. Continuity of supervision matters more than the supervisor’s grade.
Track the work. Number of repeat prescriptions handled independently. Number of discharge reconciliations. Number of audits completed. The data is what justifies the role to GP partners.
Our fully managed pharmacy technician support service covers placement, supervision and clinical oversight under a single contract. Get in touch for a deployment review.