Innovation funding sits oddly in general practice. The money is real. The routes to it are not always obvious. The application process favours practices that already have someone who knows the form. Smaller practices and PCNs without an experienced bid writer often miss the funding entirely, even where the clinical case is strong.
This piece sets out where innovation funding comes from in 2026, what evaluators look for, and where most applications fall short.
What innovation funding actually covers
Innovation in NHS funding language usually means money outside core contract funding. That covers a wide range of programmes:
- NHS England transformation funds tied to specific national priorities (cardiovascular prevention, frailty, women’s health hubs)
- ICB innovation pots, which vary by region but typically run between £15,000 and £200,000 per award
- NHS England Transformation Directorate funding for clinical software, AI tools, and data infrastructure
- Academic Health Science Network programmes
- Charity-funded programmes (BHF, Diabetes UK, Cancer Research UK) for clinical pathway redesign
- Industry partnerships where a pharmaceutical or medical device company funds service evaluation work
The clinical case is usually well-articulated by the time a practice considers applying. The challenge is matching the case to the right funding stream.
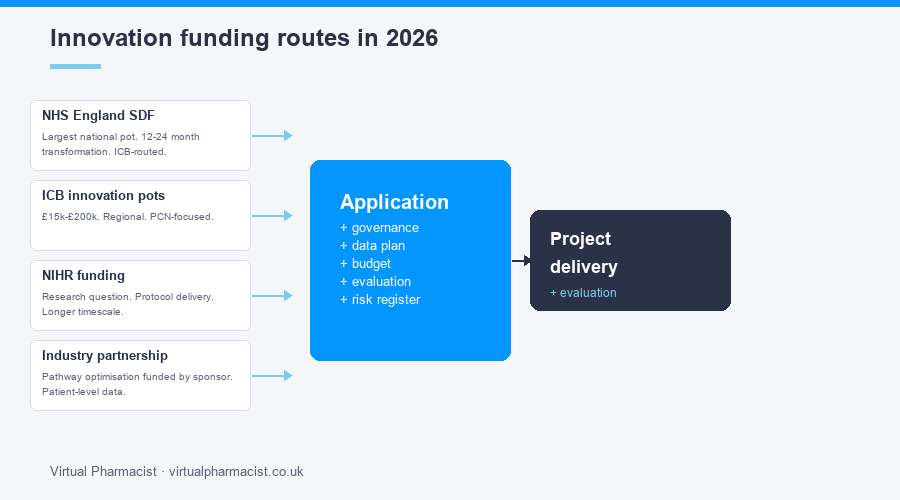
The main routes in 2026
NHS England Service Development Funding remains the largest national pot. It funds time-limited transformation work, typically 12 to 24 months, with a clear scale-up expectation. Applications go through the ICB.
PCN-level innovation funding through ARRS-adjacent streams covers workforce-related innovation. A PCN that wants to pilot a frailty service across its practices can usually find money inside the ICB rather than going national.
NIHR funding suits practices that have a research question and the capacity to deliver to a research protocol. Different administrative burden, different reporting requirements, different timescales.
Industry partnerships are the most under-used route. A pharmaceutical sponsor will fund pathway optimisation work for conditions where their drug is involved (anticoagulation, diabetes, asthma), provided the practice can show patient-level outcome data at the end.
What evaluators look for
Four things, in order.
Defined patient cohort with measurable outcomes. “Reduce cardiovascular risk in our patients” is not a cohort. “Identify the 320 patients on our list with QRISK above 20% who are not on a statin, offer a clinic, achieve a 70% statin initiation rate” is a cohort.
Realistic delivery plan. The plan has named people, named systems, named clinical pathways. It says who will do the work, how long it will take, and what could go wrong.
Evaluation built in from day one. Not bolted on at month nine. The evaluation question is set at application stage. Baseline data is collected before the intervention starts.
Scale potential. Funders are not paying for one practice’s project. They are paying for something that, if it works, can be replicated elsewhere. The application has to say what that replication looks like.
The application work that matters
The clinical case writes itself. The work that wins funding is the operational detail behind it.
Data plan. Who pulls the baseline data. From which system. Refreshed how often. Compared against what.
Governance. Information governance approval. Caldicott. Ethics where relevant. Letter of support from the ICB clinical lead.
Resource plan. How much pharmacist time. How much GP time. Admin support. IT changes. Training requirements.
Budget. Real numbers per quarter, not a single annual figure. Underspend explanation. Underspend recovery plan.
Risk register. What could fail. What the mitigation is.
A clean 30-page application with these five elements completed will outperform a 60-page application with a long clinical introduction and thin operational detail.
Where most applications stumble
Three failure modes are common.
Vague outcome targets. “Improve patient experience” sets no measurable bar. Evaluators score it as zero.
Underestimated time costs. The clinical lead is named on the project but has no protected time. The work falls between sessions. Month six shows zero progress.
No evaluation partner. Practices try to evaluate their own work, with no academic or analytical partner. Funders increasingly want to see who is doing the analysis before they release the money.
Where to get help
Our fully managed innovation funding service supports practices and PCNs end to end. Identifying the right route. Writing the application. Delivering the project. Evaluating the outcomes. Our innovation funding service covers the practical side. Get in touch if you want to talk through a specific bid.