QOF still drives a meaningful share of primary care income. It also drives some odd clinical behaviour. The indicators where pharmacist input lifts both income and clinical outcomes are not always the same as the indicators where pharmacist input lifts only income.
This piece sorts the two apart. It also covers what good QOF support from a pharmacist looks like and where practices get the support badly wrong.
What pharmacists actually shift
A pharmacist working consistently in a practice for a year typically improves performance against the following QOF clusters.
Cardiovascular indicators. Blood pressure control in hypertension and diabetes. Lipid management. Anticoagulation in AF.
Respiratory indicators. Annual asthma reviews. Annual COPD reviews. Inhaler technique audits.
Diabetes. HbA1c targets. Foot checks for high-risk patients. Albumin-creatinine ratio testing.
Mental health. Annual physical health checks for patients on antipsychotics or with severe mental illness.
Prescribing-related QOF. Items like NSAIDs in patients with CKD, antibiotic prescribing rates, hypnotic prescribing trends.
The pattern across the high-impact indicators is consistent. They require a structured patient contact every 12 months. The contact has a defined clinical content. The data has to be recorded against a specific Read or SNOMED code.
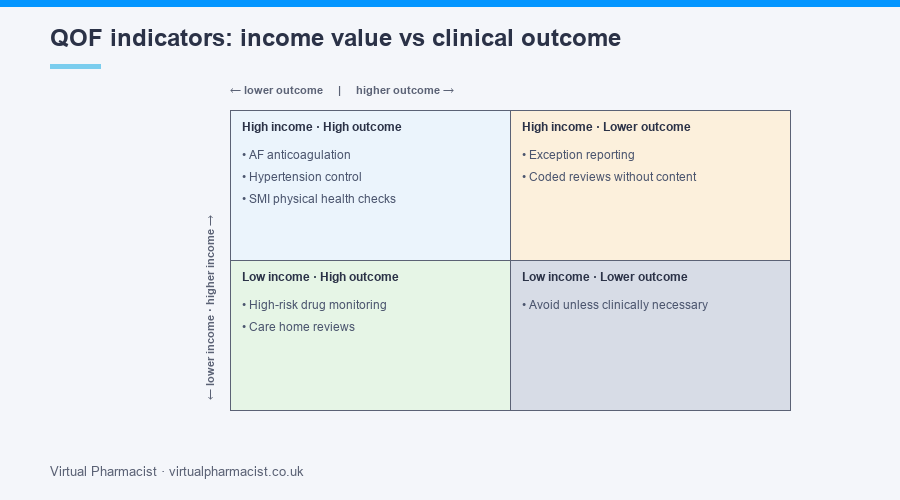
Where the income and outcome match-up is best
Three indicator clusters give both income and clinical value back at roughly the same rate.
Anticoagulation in AF. Patients with AF need a CHA2DS2-VASc score and, where indicated, an anticoagulant. Practices that systematically work through their AF register usually find 5% to 15% of patients eligible for anticoagulation who are not on one. Starting them prevents strokes. It also moves the QOF indicator.
Hypertension control. The 140/90 (or 150/90 in older adults) target is clinically defensible. Patients who get to target through pharmacist-led titration clinics have measurably better cardiovascular outcomes.
Annual SMI physical health checks. Patients on antipsychotics have shorter life expectancy. The annual physical health check catches metabolic side effects early. Pharmacists running the checks pick up issues GPs are too rushed to see.
Where the income and outcome match-up is poor
Some indicators move income without moving outcomes much.
Personalised Care Adjustment (formerly known as exception reporting). Practices that systematically exception-report patients to hit the indicator add nothing clinically. The income arrives. The patient is no better off.
Coded reviews without clinical content. A diabetes review coded against the right SNOMED but completed in five minutes adds nothing the patient could not have done at home.
Some prescribing indicators where the underlying clinical question is more complex than the indicator allows.
A pharmacist who chases all QOF income without thinking about which indicators justify the time ends up doing work that scores well on Friday’s report and badly on Monday’s morbidity.
The QOF audit cycle pharmacists run well
The work pattern looks roughly like this.
April. Pull the prior year’s data. Identify indicators where the practice is below the upper threshold but above the lower. These are the ones where extra effort still earns income.
May to August. Targeted clinics against the prioritised indicators. Patient contact pre-booked. Templates set up. Coding agreed in advance.
September. Mid-year check. Are indicator scores tracking? Are patients showing up? What is going wrong?
October to January. Catch-up clinics on indicators that are below target. Outreach to patients who have not attended. Exception report only where clinically justified.
February to March. Final push on indicators still at risk. Audit data quality. Identify next year’s improvement targets.
A pharmacist running this cycle reliably picks up 3 to 7 indicators a year that would otherwise have under-performed.
What it looks like done badly
Pharmacist asked to “do QOF” with no defined indicators. The work fragments across every indicator and improves none.
QOF clinic that runs on the day income reports are due. The clinic catches up activity but misses outcome opportunities.
GP partners not engaged. The pharmacist identifies prescribing changes but cannot get sign-off from the partners. Patients miss interventions.
Coding errors not corrected. The pharmacist does the clinical work but the wrong SNOMED gets recorded. The work happens. The income does not arrive.
Where to start
If your practice’s QOF performance has slipped, or you have a sense the income is being earned at clinical cost, the fix is structural. A defined cycle of QOF improvement work, mapped against indicators where the income and outcomes both matter, run by a clinician with the time to do the patient-facing work properly.
Our fully managed quality and audits service covers QOF audit and improvement work end to end. Get in touch for a baseline assessment.